Reading Assignment: Chapter 21
Respiratory Defenses
I. Lining—
{kind=link}
1. mucus–trapping; if dry–cystic fibrosis or a disease called atrophic rhinitis then-ineffective
2. cilia–sweeping –action compromised by narcotics, smoking
II. Filtering–shape, hair–aeordynamics
droplet size
{kind=link}
defenses:
Bronchis and bronchioli associated lymphoid tissue = BALT
alveoli = gas exchange / resident macrophages
{kind=link}
lung — unique blood supply
– “foreign” materials susceptible to lodging in lungs
Normal biota: found in most people with no overt disease
colonization–establishment of a critical self sustaining number of organisms in an anatomical site
SO Infection is colonization in a normally sterile site
Disease: pain! and / or tissues destroyed or function harmed
Virulence
attachment
ability to avoid immune, circumvent defenses
invasion
Koch’s Postulates [see Nester appendix, current edition-p419]
1. bug present in all cases
2. pure isolate
3. inject into a normal animal & cause disease
4. re-isolate THE organism
[limits: if organism cannot be cultured in the lab; if unethical to test model in humans and animal models are also not available]
Molecular Postulates
- virulence factor or its product must be present in pathogens
- intro of cloned gene should change a non-pathogenic strain into a virulent one and disruption of the gene in the pathogen should convert it to a non-pathogen
- The genes for virulence must be expressed during the disease process
- Antibodies or immune cells specific for the virulence gene products should protect.
Normal Biota
Streptococci
Moraxella
Diphtheroids
Bacteroides
Staph
{kind=link}
Pathogens of the Upper Respiratory system:
Streptococci G+ round, chains; catalase negative
several ways to type the many Strep; one is by
{kind=link}
Hemolysins–
– 1. non hemolytic strep [no lysis of red blood cells-rbc]
– 2. a hemolytic strep [incomplete lysis, veridans group]
– 3. b hemolytic strep [complete lysis]
diseases include scarlet fever, rheumatic fever, kidney disease
{kind=link}
{kind=link}
{kind=link}
another is by
{kind=link}
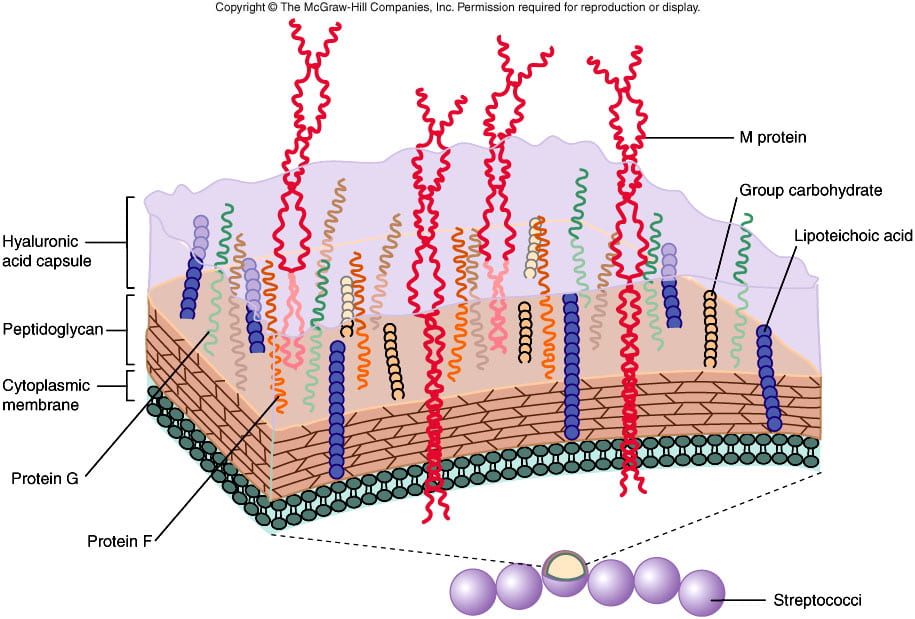
Virulence factors of Strep pyogenes
S. Pyogenes is b-hemolytic [this is also called group A strep]
capsule -made of hyaluronic acid identical to host connective tissue
{kind=link}
This capsule is anti-phagocytic and non-immunogenic
pyogenes– means pus former.
Has many virulence factors:
M protein — avoid phagocytosis & C’ binding [degrades C3b] by binding factor H [H protein is made by humans and it regulates complement by degrading C3b].
{kind=link}
F protein — allows for binding to fibronectin and thus to epithelial cells of pharynx and skin
G protein–like the protein A of Staph aureus blocks the Fc portion of antibody
Enzymes:
{kind=link}
C5a peptidase [degrades C5a]
HyaluroniDASE-degrades and separates epithelium by its hyaluronic acid
Streptokinases — lyses blood clots
DNAse together with Hyaluronidase and Streptokinase allow the bugs to travel in the host.
Toxins:
Pyrogenic toxins–also known as [aka] erythrogenic toxins–skin rash, scarlet fever and fever
Streptolysins are cell killers (host cells die)
Streptolysin O– inactivated by cholesterol and oxygen, immunogenic
Streptolysis S non-immunogenic
both lyse white cells [aka luekocytes],platlets, rbc, augment release of lysosomal enzymes
more Path:
T cells and antibodies are made against M protein, this is protective.
B ut in some cases Rheumatic fever — inflammation of the heart–valvular
also antibodies react against joints [of some]–arthritis
glomerulonephritis
These are cross reactions between M protein & self components–heart, joint that occur at the level of the T cell which sees MHC+ peptide [foreign preferably!] as antigen
{kind=link}
{kind=link}
Corynebacterium diphteriae
G+ rod
dead white membrane
DT exotoxin:heart, kidney, nerve & muscle have highest # receptors for DT
Reaction
Inhibition of all protein synthesis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Vaccine against toxin itself is effective in preventing disease.
Common colds: Viral infections [Adeno and Rhinovirsuses]
Rhino viruses attach to ICAM-1 [intracellular adhesion molecule]. This molecule is used to bring in the host’s defending cells.
{kind=link}
Self-limited -grow at 33 degrees not at 37 degrees.
While these viral infections most often go away [antibodies, interferon], a viral infection often enhances suseptibility to bacterial infections.
cilia lose function
or added to by man-made reasons–antibiotics killed the normal biota–surface avaialable
some bacteria use viral proteins to attach to host cells.
Why do viral common colds recur?
1. different viruses 100 adenoviruses, 42 known to infect humans, 100+ serotypes amongst these]
2. rhinoviruses change their antigenic structure by mutations.
Go to notes on DEFENSES
Streptococcus pneumonia a.k.a. diplococcus pneumonia
{kind=link}
pathology–alveloi swell, G+
– THICK capsule
phagocytosis by “streaming” requires friction
80 different strains–by different capsules, attempt to “eat”–
vessel dilation
more phagocytes
serum
dead bacteria & PMN + macrophage
even more fluid= exudation
normal x-ray the lung is black
alveoli — fluid filled — gray — white patches= consolidation
{kind=link}
infection spread by:
1. contiguity
2. blood stream — inflamed heart lining=endocarditis
– meningitis & septicemia
spread helped by–>neuraminidase–>(virulence factor)
Antibody — Capsular Polysaccharides
erythromycin — resistant strains
Klebsiella — G- rod
endotoxin damage of tissue
–>release continues after death of Klebsiella
Fibrous collagen
ubiquitous & major source of
R factors = plasmid
{kind=link}
Walking Pneumonia — mycoplasma in respiratory tissue
antibiotics such penicillin, cephalosporins do not work [why?]
Viral Broncho-Pneumonias — symptom–cough
{kind=link}
{kind=link}
Bordetella Pertussis
Hughes Bordet
burst of lung into pleura called pneumo thorax
attachment
Bordetella Pertussis — ciliated epithelia of trachea
attachment: 1. hemagluttnin– 2. pertussis toxin
{kind=link}
toxins:
1. toxin 1 kills cell tracheal lining
2. pertussis toxin released upon B. pertussis death.
Pertussin toxin: ADP — ribosylates a GDP binding protein
the effect is loss of pump control for salt & water
an “AB” toxin — binding — allows entry into cell — targeting
action = “catalytic domain” toxicity
{kind=link}
Pertussis toxin–in the U.S.
235,000 cases/yr 1934
1,000 cases/yr 1981
6,000 cases/yr 1988
Whooping Cough — tracheal bronchitis; major child-killer 5-30% mortality if no vaccine
Summarizing:
Virulence Factors
1. hemaglutinin
2. pertussis toxin
– ADP-ribosylates a GDP binding proteins
One new prevention attempt: Vaccinate the grandparents
{kind=link}
INFLUENZA
orthomxyo family
ss RNA
segmented genome
antibodies prevent infection
{kind=link}
Virulence Factors:
Hemagglutinin – allows virus to stick to cells
Neuraminidase – rip off obstructing sugars, enhances attachment and *detachment when departing cell.
– airway infection NOT airsacs
– results in broncho pneumonia or bronchitis
inflammation by macrophages (not by PNMs)
living cells die: 1. can’t make protein
2. NK and cytotoxic T cells [the T cells see the nucleoproteins of flu virus]
desquamation — easy for 2° infections
by S. aureus or Strep. pn or H. influenza
viral infection spreads–muscle
secondary complications– liver
Reye’s syndrome
nervous system — viral encephalitis (brain inflammation)
Guillian-Barre syndrome — peripheral nerves
Evolutionary–genetic mechanisms
Antigenic drift
Epidemic
changes through point mutations
{kind=link}
Another illustration of shift and drift mechanisms
{kind=link}
Pandemic = global epidemic, 1 every 10 – 20 years
Histoplasmosis: Histoplasma capsulatum,
bird droppings
has a capsule but not as spoken of in the bacterial sense [that is, a bacterial capsule is a glycocalyx that is distinct and gelatinous and is often positively correlated with an organisms ability to cause disease] instead what the namers of this organism were referring to was the mold phase in which those coatings around the asexual spore with projecting knobs are more propoerly referred to as large conidia[so these notes reinforce the namers intention and the Nteser text says” no capsule.]”
{kind=link}
{kind=link}
{kind=link}
immune response: granuloma formation=a Th1 response
Coccidiodomycosis by Coccidioides immitis
dimorphic, aerobic
grows saprolytically [on dead matter,] mold form-25 degrees C
unicellular = yeast forms, ball of cells 37 degrees C
{kind=link}
desert living
H. capsulatum and C. Immitis can cause an IgE response=a Th2 response
activating basophils & mast cells–histomine, serotonin, & others = allergy can become chronic disease
{kind=link}
Legionella pneumophilia – odd lipids, hard to see at all by Gram stain
fastidious, fine aerosols
{kind=link}
encourages phagocytosis by having a porin protein that binds to C3b
Macrophages — prevents: fusions of the phagosome with the lysosome
b-lactamase so resistant to penicillin and cephalosporins
Hantavirus
aka: 4 Corners virus 1993 or Meuto Canyon virus or Sinombre virus
casues acute hemorrhagic pneumonia
animal reservoir — rodents
Hanta is a hemorrhagic fever like Ebola 🙂
{kind=link}
{kind=link}
Ebola: Lessons from a survivor
also like (lasa, marburg, rift valley fevers but these however target the kidney)
SARS see other link!
Middle East respiratory syndrome coronavirus (MERS-CoV) has emerged as a highly fatal cause of severe acute respiratory infection. Since April 2012, 1,348 cases and 479 deaths in over twenty-five countries have been attributed to this novel beta-coronavirus
Tuberculosis
acid fast, long rod shaped bac.
8 million new cases /yr worldwide
3 million deaths/yr
400,000 + 5% 2° to HIV infections
Koch’s Disease Mycobacterium tuberculosis, MtbCell wall and slow growth rate
Cell wall
lots of lipids: waxes, mycosides, glycolipids
– 25% dry wt. arabogalactans [carbohydrates]
fatty acids/mycolic acids= water repellant, resistant to water soluble disinfectants
{kind=link}
acid fast, once stained — stay stained, can’t decolorize = AF1.
Mycolic acids–one called cord factor is associated with virulence
1. looks like a cord, geometry
2. slow growth rate, aerobic, requires enriched media, doubling rate is 10 -100x slower –>
3-8 wks for colonies, 12-24 hr to divide
Runyon Classification
5 GROUPS
rapid growers [group IV]; M. fortuitum, grow in days
photochromogens [group I]; M. Kansasii, pigment when grown in light
scotchromogens [group II]; M. gordonae, pigment even if grown in dark
slow growers [group III] M. avium intracellidaire , disseminated disease causing,– grow in two weeks
Sub-group of slow growers — called the Mtb complex
M. tuberculosis} lung disseminated disease
M. bovis
M. leprea
tb infectious courses: Steps summarized
macrophages — phagocytose Mtb
Mtb escapes — inhibits phagolysome fusion
cell wall, has muramyl dipeptide
stimulates macrophages to make and secrete inflammatory factors
–>improve T responses
IFNg and other activated Th1 cell products act on macrophages
{kind=link}
to make antibodies researchers add Mtb that is killed — adjuvant [any substance which increases the immune response to another substance]
Typical Mtb pathology
1. intense inflammatory reaction
2. even activated macrophages aren’t efficient killers of Mtb
Immunity arises late
debris & build up } caseation — “cheese making”
lesion in lung called a granuloma
{kind=link}
progression of Mtb
3. systemic — wasting due to reducing muscle mass
{kind=link}
treatment of slow growers — prolonged, high doses of antibiotics
Testing for tb vs immunizing with BCG
{kind=link}
alternative blood test that looksfor ifn-g made to tb antigens
Effect of Immune STATUS
1st exposure
Primary Complex — children
normal small lesions, self-limited, initiates immune memory, skin test & to PPD (protein in cell wall of Mtb)
Full blown tb
path due to immune response
second time is worse
Immumocompromised — if infected with Mtb
1. little pathology, few granulomas
2. spread all over, small low grade abcesses
high Mtb load — fatal
called miliary tb